***Secondary causes of esophageal eosinophilia: gastroesophageal reflux disease, eosinophilic gastrointestinal disease, achalasia, hypereosinophilic syndrome, esophageal Crohn’s disease, infections (fungal, viral), connective tissue disorders, autoimmune disorders, vasculitis, drug hypersensitivity reactions, pill esophagitis, stasis esophagitis, graft versus host disease, Marfan syndrome type II, hyper-IgE syndrome, PTEN hamartoma tumor syndrome, Netherton’s syndrome, severe atopy metabolic wasting syndrome.
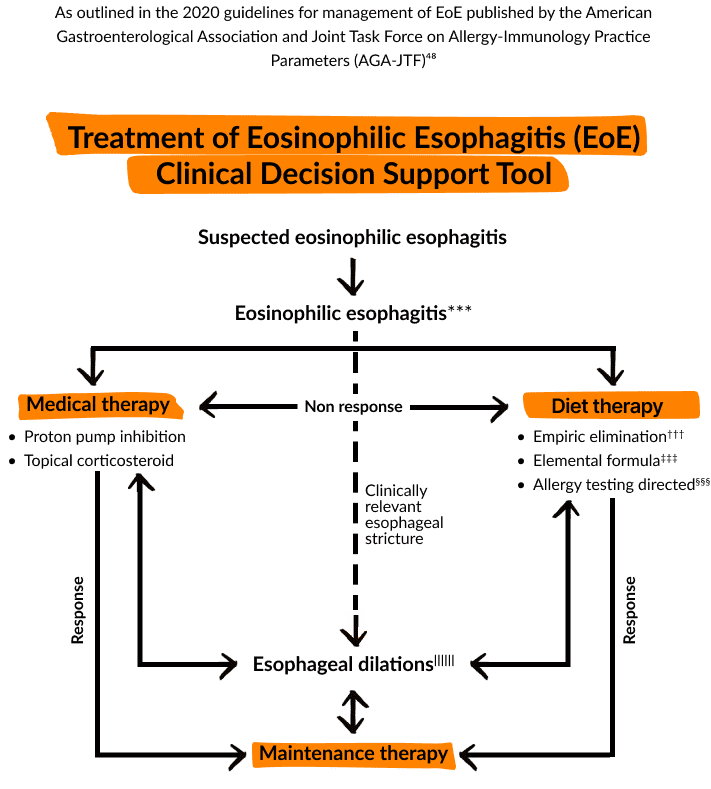
†††Recommendation in favor of empiric elimination diets is based on the published experience with the six food elimination diet (SFED). Patients who put a higher value on avoiding the challenges of adherence to diet involving elimination of multiple common food staples and the prolonged process of dietary reintroduction may reasonably decline this treatment option. Emerging data on less restrictive diets (4 food, milk elimination, 2-4-6 step up diet) may increase both provider and patient preference for diet therapy.
‡‡‡Patients who put a higher value on avoiding the challenges of adherence to an elemental diet and the prolonged process of dietary reintroduction may reasonably decline this treatment option.
§§§Due to the potential limited accuracy of the currently available, allergy based testing for the identification of specific food triggers for EoE, patients may prefer alternative medical or dietary therapies to an exclusively testing-based elimination diet.
||||||Esophageal dilation does not address the esophageal inflammation associated with eosinophilic esophagitis.