Uncover the signs of chronic, relapsing esophageal inflammation across the 3 domains of EoE: symptoms, endoscopy, and histopathology.1-4 symptoms, endoscopy, and histopathology.1-4
SEE EoE BEYOND
Symptoms
~50% of dysphagia cases may not be reported to a clinician, and it is the most common symptom of EoE, according to a 2018 online survey.*1,3-5 Patients may develop adaptive behaviors that mask symptoms, making EoE difficult to diagnose by symptoms alone.3,4,6,7
*In an April 2018
SEE EoE BEYOND
Endoscopy
EoE should not be ruled out based on endoscopic findings alone. In a 2007 retrospective study of 117 patients with EoE, 1 in 4 had normal endoscopic findings.†8
†Of 117 patients with EoE, the esophageal mucosa was regarded as normal in 24.8% of the patients.8
SEE EoE BEYOND
Histopathology
Without investigating symptoms and endoscopic findings, the histological presence of esophageal eosinophilia alone does not establish an EoE diagnosis.3
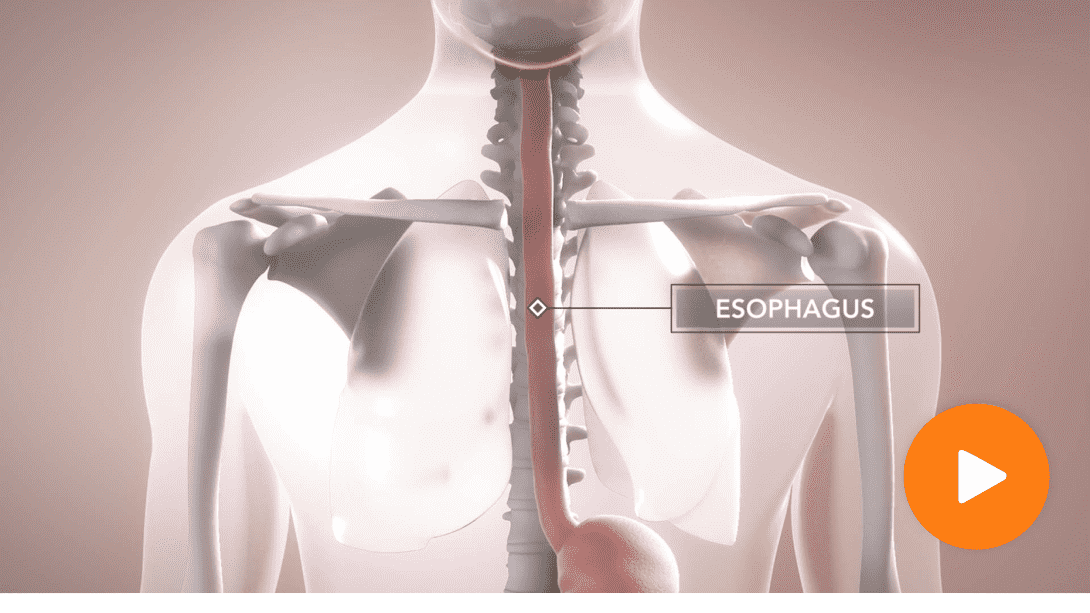
EoE is an inflammatory disease marked by the elevated presence of eosinophils localized in the esophagus2,9
EoE is a chronic, immune-mediated disorder in which eosinophils accumulate in the esophagus, causing inflammation and edema to the surrounding tissue.9,10 Eosinophils are not typically found in the esophagus under normal circumstances.9 In EoE, however, an immune response to food allergens or aeroallergens increases the number of eosinophils in the esophagus along with other inflammatory immune cells.11
EoE impacts patients in many different ways9,12,13
In addition to symptoms like dysphagia, untreated chronic inflammation can manifest in endoscopic complications like strictures, horizontal rings, and furrows.10,14,15 Some patients with EoE may also present with psychiatric comorbidities.13 One 2020 retrospective study of 883 patients found that up to 28% of patients with EoE experienced psychiatric comorbidities such as anxiety (23%) and depression (17%).‡13
EoE involves the complex interplay of genetics, environmental factors, immune system dysfunction, and atopy16
Some patients with EoE have a history of IgE-mediated allergic comorbidities, with sensitivity to food or other allergens in the esophagus.3,17-20 Esophageal inflammation and remodeling in EoE may be a result of repeated exposure to food and environmental allergens that can eventually lead to impaction of solid or coarse foods, which may not necessarily contain those inflammation-triggering allergens.17,18 Educating your patients about the consequences of this ongoing inflammatory process is important.
‡In a study using the University of North Carolina EoE Clinicopathologic Database from 2002 to 2018. Of 883 patients diagnosed with EoE (per consensus guidelines), 241 (28%) had a psychiatric comorbidity. Study limitations include that this is a single-center retrospective study where a comparison to the national representative figures was done through nonstatistical analyses.13
The mechanism of disease in EoE
The prevalence
of EoE is rising21-23

Approximately 1 in 2000 people in the U.S. live with EoE14,17,22-24
The majority of EoE cases are in children, adolescents, and adults ages 50 or younger, but it can affect all ages.1,3,14,25,26
EoE is approximately twice as common in men vs women and more common among Caucasians, but can affect all sexes and races14,25,26
EoE is a leading cause of dysphagia and food impaction for children and young adults3
Emerging evidence suggests environmental factors such as microbes, early life events affecting the microbiome, and other factors may be contributing to the rise in prevalence of EoE11,17,21,27-29
One 2020 retrospective study of 883 patients reported that one-third of adults and 1 in 7 children with EoE have received a diagnosis of a psychiatric condition§13
§In a study using the University of North Carolina EoE Clinicopathologic Database from 2002 to 2018. Of 883 patients diagnosed with EoE (per consensus guidelines), 241 (28%) had a psychiatric comorbidity. Study limitations include that this is a single-center retrospective study where a comparison to the national representative figures was done through nonstatistical analyses.13
Adaptive behaviors can contribute to disconnects in what patients say and what their endoscopies show1,3,11,28
For patients with EoE, inflammation can lead to symptoms such as dysphagia and food impaction, which may produce a certain amount of fear and interfere with everyday life.9 Without realizing, some patients develop adaptive behaviors to cope with these symptoms.6,28 But adaptive behaviors can minimize awareness and symptom reporting, so symptoms of EoE should always be assessed in conjunction with endoscopies and biopsies.3,4,6,28
Identify adaptive behaviors to help reveal EoE||
Chewing food excessively3,28,30
Eating slowly7,28,30

Cutting food into small pieces1,11
||Illustrative only. Adaptive behaviors will vary by patient.
Asking the right questions can identify adaptive behaviors
and potentially reveal masked symptoms of EoE1
SEE EoE THROUGH 3 DIAGNOSTIC DOMAINS:
Symptoms, Endoscopy, Histopathology
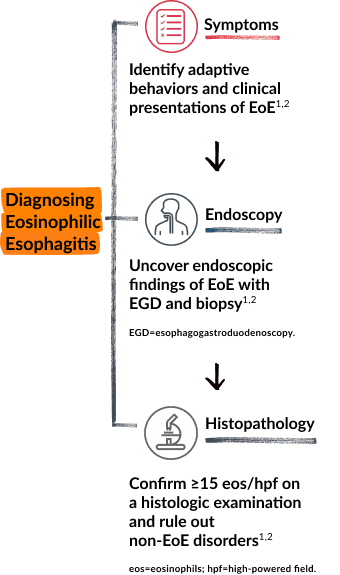
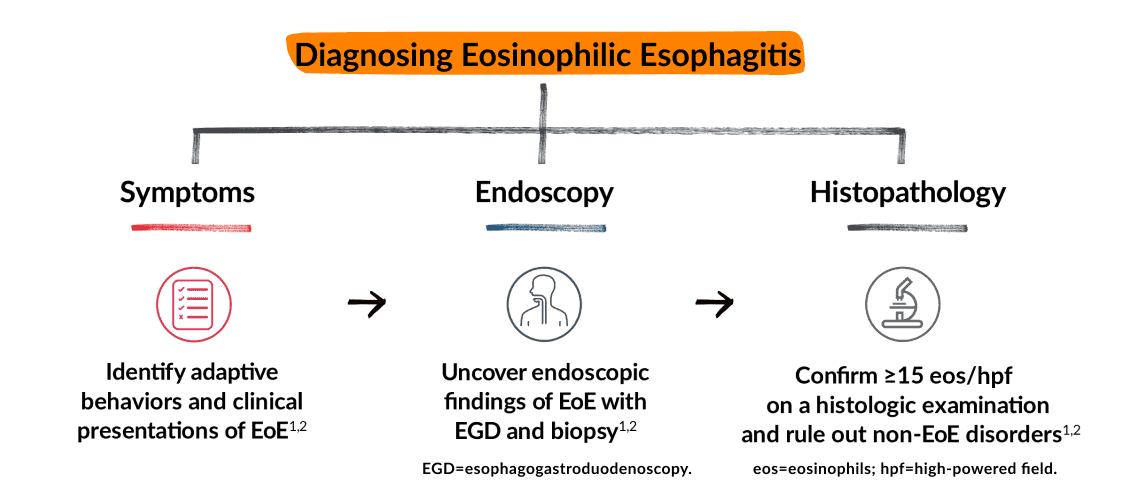
According to guidelines, diagnosis and monitoring of EoE require the holistic approach of assessing the 3 domains together¶2-4,28
There are several limitations associated with each of the 3 domains so no single domain alone should be relied on to draw conclusions about diagnosis, or how to manage ongoing disease activity.2-4,28 EoE is heterogeneous and can have overlapping signs and symptoms with other eosinophilic conditions, reinforcing the need for a differential diagnosis through the 3 domains.2
¶As per the 2018 updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis from the A Working Group on proton pump inhibitor–responsive esophageal eosinophilia (AGREE) Conference.
SEE EoE THROUGH 3 DIAGNOSTIC DOMAINS:
Symptoms, Endoscopy, Histopathology Symptoms, Endoscopy, Histopathology
According to guidelines, diagnosis and monitoring of EoE require the holistic approach of assessing the 3 domains together¶2-4,28
There are several limitations associated with each of the 3 domains so no single domain alone should be relied on to draw conclusions about diagnosis, or how to manage ongoing disease activity.2-4,28 EoE is heterogeneous and can have overlapping signs and symptoms with other eosinophilic conditions, reinforcing the need for a differential diagnosis through the 3 domains.2
¶As per the 2018 updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis from the A Working Group on proton pump inhibitor–responsive esophageal eosinophilia (AGREE) Conference.
SEEING EoE BEYOND
Symptoms
In a 2018 cross-sectional U.S. online survey of 31,129 people, 1 in 6 adults reported experiencing dysphagia (difficulty swallowing).#5 In adults with EoE, dysphagia is the most frequently reported symptom.1,7 Symptoms like dysphagia can generate fear, embarrassment, and distress for patients, which brings additional complexity to their struggle with the disease.9
Beyond dysphagia, EoE presents with a variety of symptoms across all ages.1,25 Understanding how symptoms may vary between age groups can be helpful when assessing clinical manifestations of EoE.1,14 Family history of EoE or dysphagia should increase the clinical index of suspicion.2
#In an April 2018 Takeda-sponsored cross-sectional,
Common symptoms of EoE**28
Adults
- Difficulty or pain when swallowing
- Food getting stuck in esophagus
- Heartburn that does not respond to medicine
- Swallowed food coming back up
- Abdominal, chest, or throat pain
- Avoiding certain foods that trigger symptoms
Children
- Difficulty or pain when swallowing
- Choking sensation
- Food getting stuck in esophagus
- Abdominal, chest, or throat pain
- Nausea and vomiting
- Disrupted sleep
- Loss of appetite
Infants and Toddlers
- Food aversion
- Vomiting
- Choking while eating
- Disruptive sleep
**Individual symptoms will vary by patient.
Limitations of symptoms alone Limitations of symptoms alone
If your patient is suffering from symptoms of EoE, consider an endoscopy with biopsies to help assess esophageal inflammation and confirm suspicions of EoE.1 Some patients may present with symptoms that do not correlate with endoscopic and histologic findings because they can be masked by adaptive behaviors or overlap with other conditions.3,28,33 Learn more about adaptive behaviors, or scroll to see EoE beyond endoscopy.
SEEING EoE BEYOND
Endoscopy
Esophageal remodeling driven by inflammation can manifest as endoscopic features that can vary
by age3,34
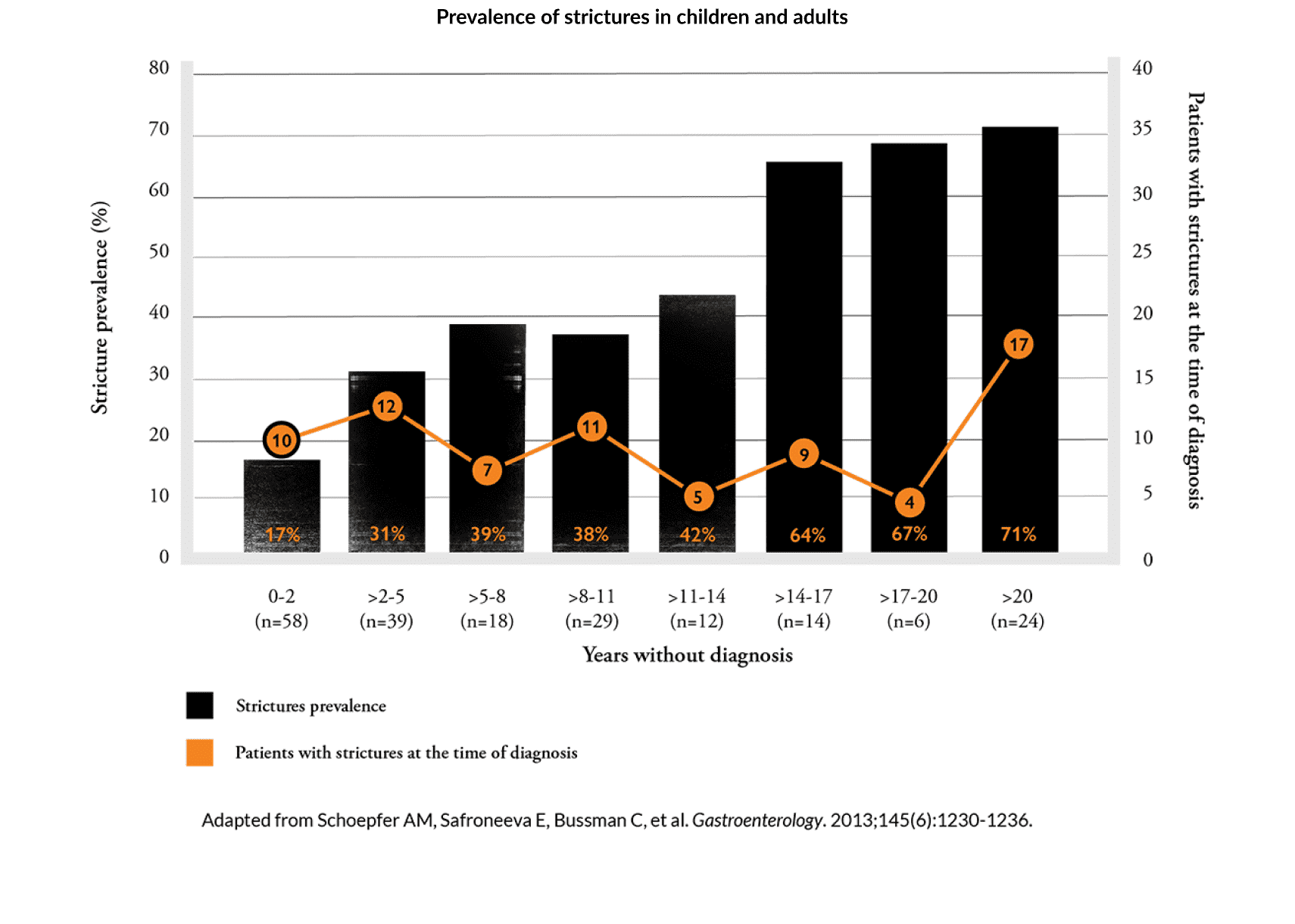
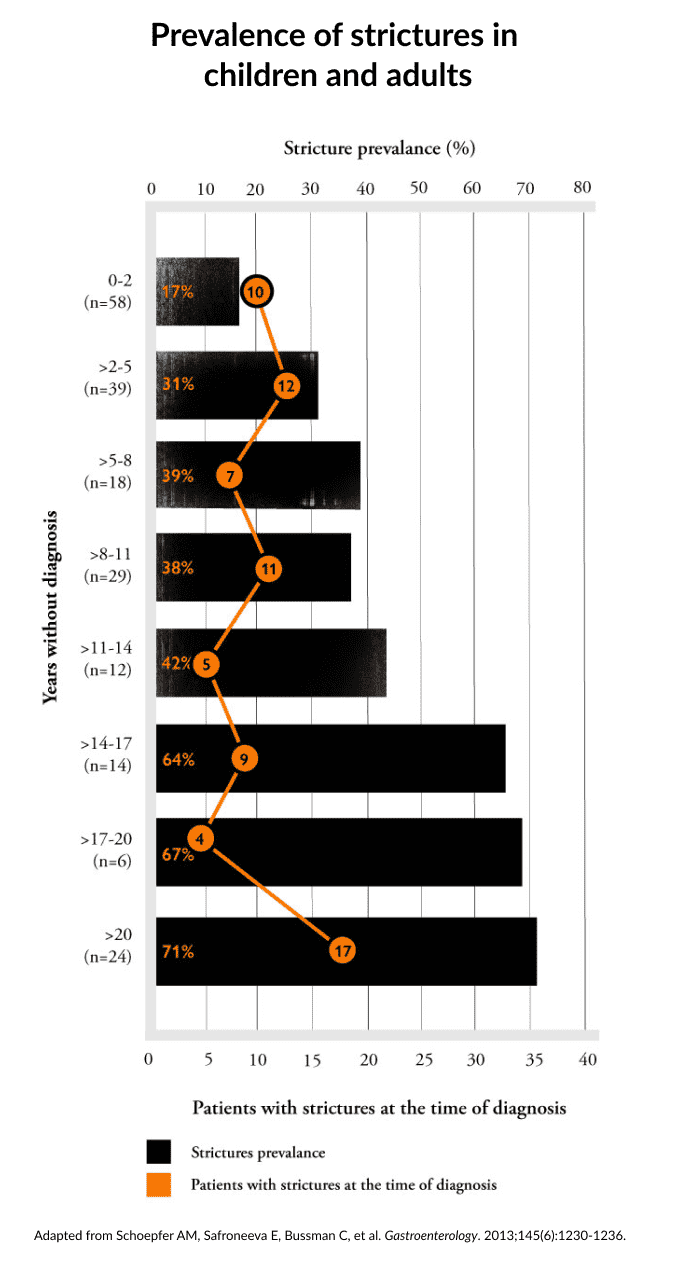
Data in adults suggest that there's potential for inflammation to progress into strictures in some EoE patients with untreated disease.18,35
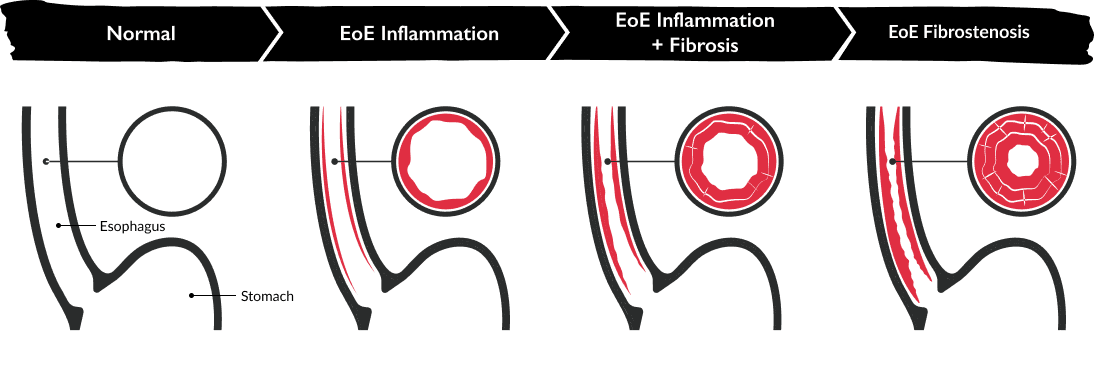
Illustration adapted from Dellon ES, Hirano I. Gastroenterology. 2018;154(2):319-332.e3.
In adults, esophageal remodeling can manifest as fibrostenotic complications, such as strictures, which can lead to food impactions.12,34,36 For infants and toddlers, remodeling can lead to food avoidance.1,3 In children, endoscopic features like edema and exudates are more commonly seen.12,34,36 Diagnostic delays may increase the risk of fibrostenotic complications.10,12
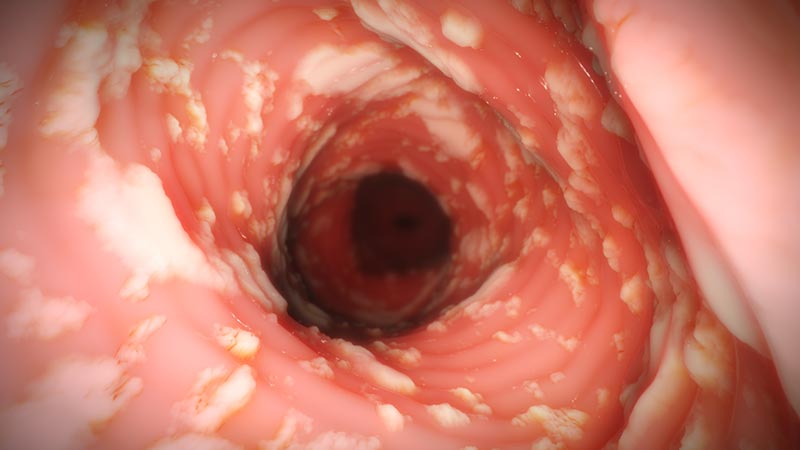
Assessing endoscopic severity of EoE through 5 key features
There are 5 key endoscopic features–edema, rings, exudates, furrows, and strictures–that have been well studied and validated to help assess the endoscopic severity of inflammation and fibrostenotic remodeling in EoE across all ages.3,12,28,37,38 Though endoscopic findings are well documented in EoE, they cannot reliably establish a diagnosis on their own.3,37
Edema

- Swelling of the esophageal mucosa3,28,39
- Thick and whitish appearance28,39
- Decreased vascularity3,39
- May be more common in children34,36
Horizontal Rings

- Formation of multiple rings28
- Can appear fine, web-like, or thickened28
- Also termed trachealization or the "corrugated/ringed" esophagus28
- May be more common in adults34,36
Exudates
- Patches of whitish papules28
- Often 1-2 mm in diameter28
- Resembles esophageal candidiasis28
- May be more common in children34,36
Furrows

- Vertical esophageal lines or ridges in the esophageal wall28
- May be more common in children34,36
Strictures

- Narrowed esophagus, usually <13 mm diameter3,33
-
- Featureless, unchanging column28
- Poor expansion on air insufflation28
- Proximal and/or distal stenosis28
- Can cause food impactions and block endoscope40
- May be more common in adults34,36
- Edema
- Horizontal Rings
- Exudates
- Furrows
- Strictures
Edema
- Swelling of the esophageal mucosa3,28,39
- Thick and whitish appearance28,39
- Decreased vascularity3,39
- May be more common in children34,36
Horizontal Rings
- Formation of multiple rings28
- Can appear fine, web-like, or thickened28
- Also termed trachealization or the "corrugated/ringed" esophagus28
- May be more common in adults34,36
Exudates
- Patches of whitish papules28
- Often 1-2 mm in diameter28
- Resembles esophageal candidiasis28
- May be more common in children34,36
Furrows
- Vertical esophageal lines or ridges in the esophageal wall28
- May be more common in children34,36
Strictures
- Narrowed esophagus, usually <13 mm diameter3,28
-
- Featureless, unchanging column28
- Poor expansion on air insufflation28
- Proximal and/or distal stenosis28
- Can cause food impactions and block endoscope40
- May be more common in adults34,36
Internal images of the body are artistic representations. Endoscopic features will vary by patient.
Limitations of endoscopy alone Limitations of endoscopy alone
Due to the patchy nature of the disease, some patients with EoE can present with normal endoscopic findings.1-4 Endoscopies can miss complications, such as strictures, caused by chronic inflammation in EoE.41 Endoscopic findings should be assessed in conjunction with symptoms and histopathology.1-4 Scroll on to see EoE beyond histopathology.
SEEING EoE BEYOND
Histopathology
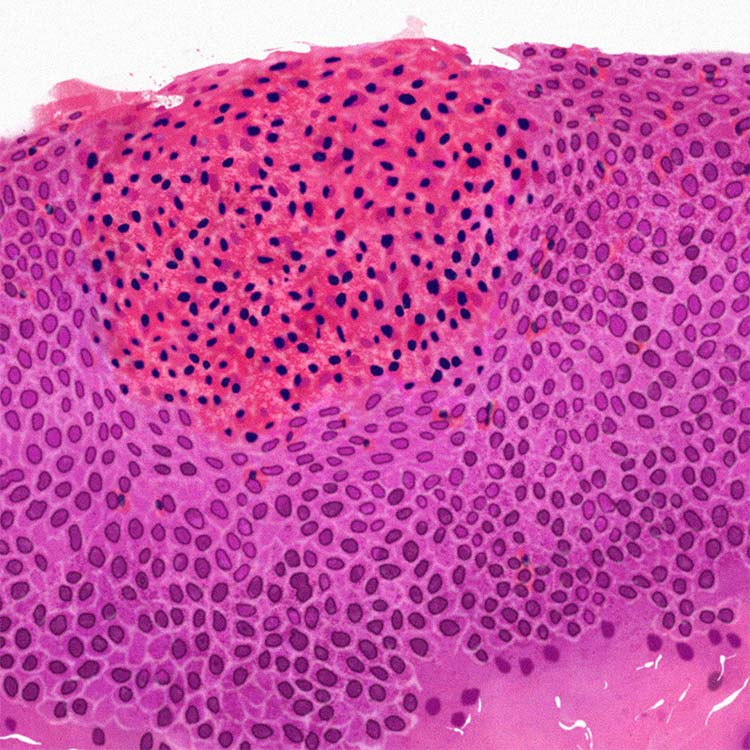
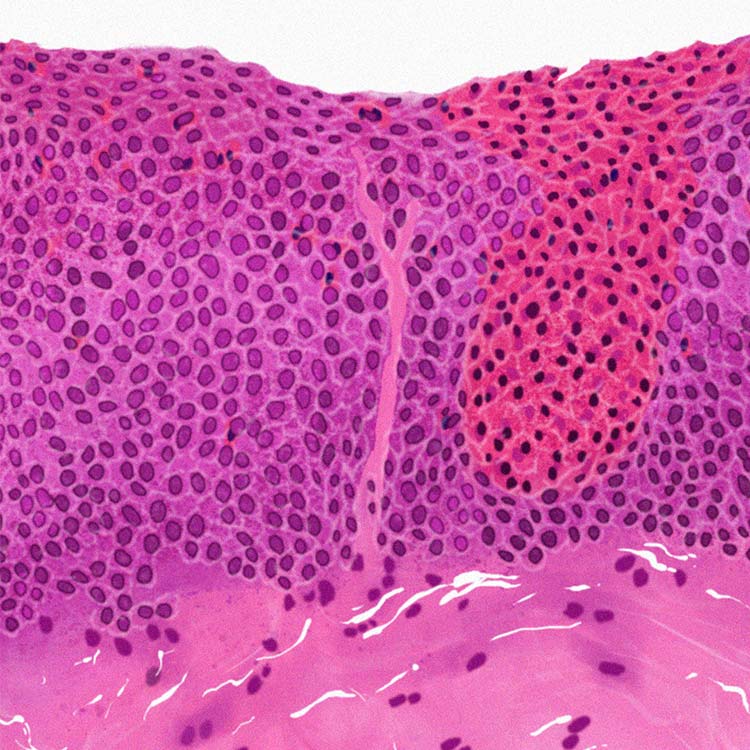
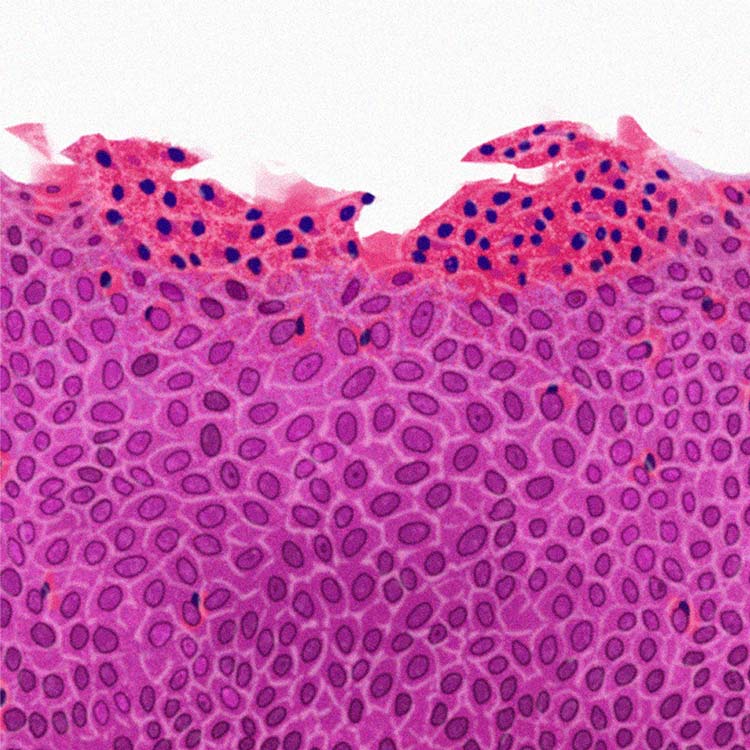
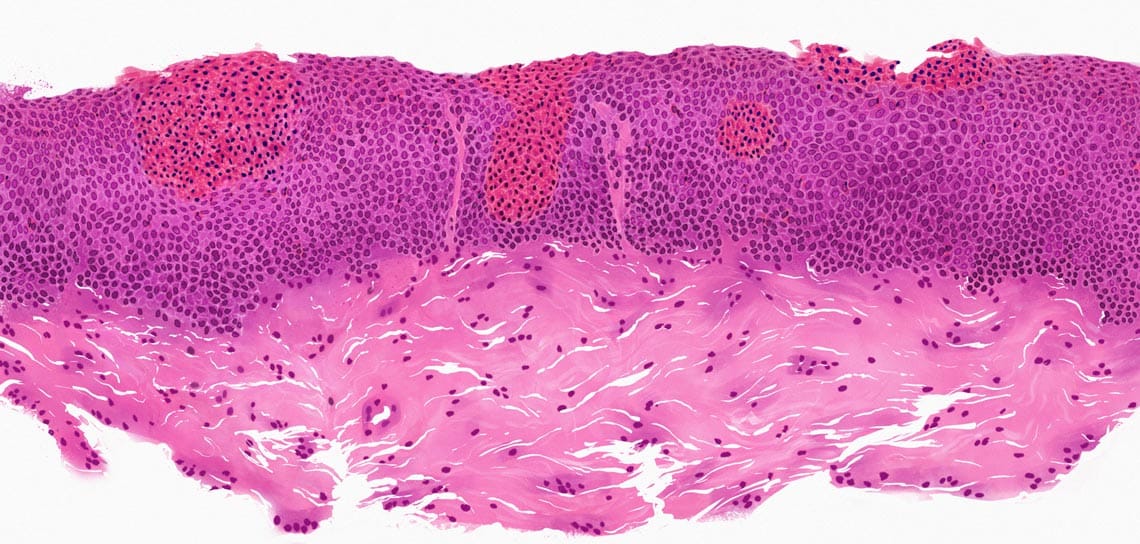
Chronic inflammation in EoE can be found inside the esophageal tissue, where eosinophils and other cells can cause recruitment of additional inflammatory immune cells, which contribute to tissue damage of the esophagus.10,11,18
The guidelines from the 2017 AGREE conference indicate that an eosinophil count of ≥15/HPF (high-power field) in at least one of multiple esophageal biopsy samples taken from different locations is clinically indicative of EoE.2,3 The presence of esophageal eosinophilia alone, however, cannot establish an EoE diagnosis without further investigation of symptoms and endoscopy.2-4
See inflammation beyond eosinophils2,3,42 See inflammation beyond eosinophils2,3,42
Other histologic features can help assess the severity and extent of esophageal inflammation. The interactive tissue below can help reveal other markers of inflammation.
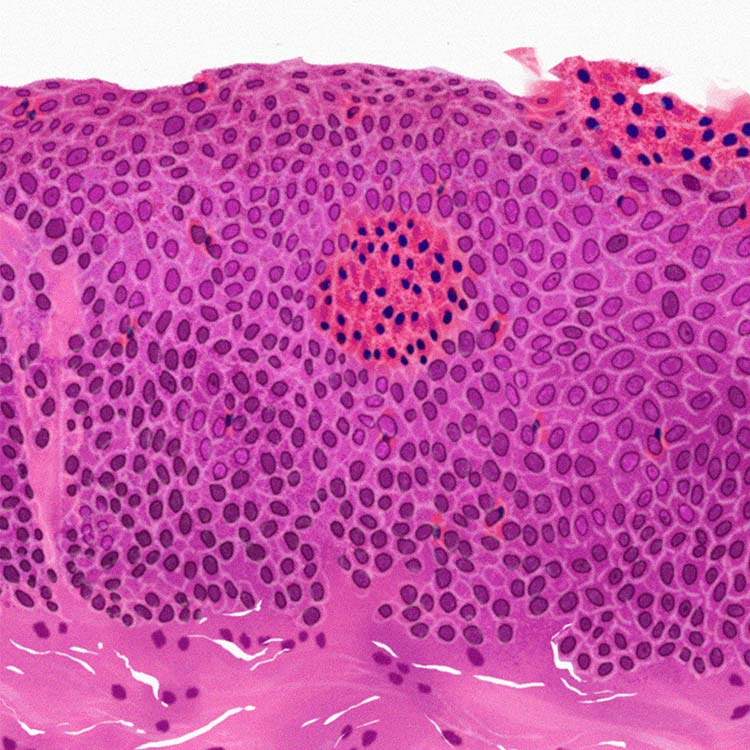

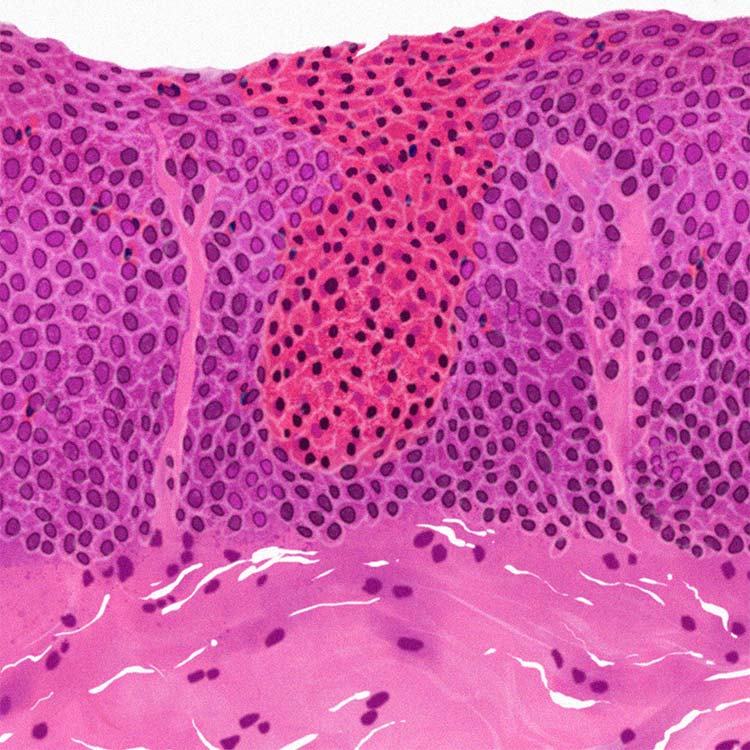
Basal zone hyperplasia (BZH):
>15% of the epithelial thickness3,11,42
Papillary elongation:
Papillae extend above the mid portion of the squamous mucosa.3,11,43 Also observed in GERD.43
Lamina propria fibers (LPF):
Thickened connective tissue fibers in the lamina propria3,42
Dilated intercellular spaces (DIS):
Spaces around squamous epithelial cells that exhibit intercellular bridges3,11,42
Eosinophil inflammation (EI):
Eosinophil count within the most densely populated HPF (high-power field)3,11,42
Internal images of the body are artistic representations. Histologic features will vary by patient.
Internal images of the body are artistic representations. Histologic features will vary by patient.
Limitations of histopathology alone Limitations of histopathology alone
Histopathology may help confirm a suspected diagnosis, but esophageal eosinophilia can be a sign of various esophageal-related diseases besides EoE, like eosinophilic gastritis and GERD.2 Moreover, due to patchy infiltration of eosinophils along the esophagus in EoE, multiple biopsies should be taken from distal, mid, and proximal locations.2,3,44
Investigate all 3 domains of EoE to reduce delays
in diagnosis and help manage EoE over time2,3
According to the 2018 updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis from the AGREE Conference, PPIs are no longer a tool to diagnose EoE.2
Rationale for changing the EoE diagnostic criteria changing the EoE diagnostic criteria and removing the PPI trial2:
- Similarities between EoE and proton pump inhibitor–responsive esophageal eosinophilia (PPI-REE)
- EoE and GERD are not necessarily mutually exclusive
- Lack of a criterion standard for GERD diagnosis
- Novel mechanisms of action of PPIs to explain response of eosinophilia
- Observation that PPI-REE could also respond to classic EoE treatments
- Concern about using a treatment response to define a disease
A better standardization
for diagnosis
- Muir AB, Brown-Whitehorn T, Godwin B, et al. Clin Exp Gastroenterol. 2019;12:391-399.
- Dellon ES, Liacouras CA, Molina-Infante J, et al. Gastroenterology. 2018;155(4):1022-1033.e10.
- Lucendo AJ, Molina-Infante J, Arias A, et al. United European Gastroenterol J. 2017;5(3):335-358.
- Safroneeva E, Straumann A, Coslovsky M, et al. Gastroenterology. 2016;150(3):581-590.e4.
- Adkins C, Takakura W, Spiegel BMR, et al. Clin Gastroenterol Hepatol. 2020;18(9):1970-1979.e.2.
- Putnam PE. Gastrointest Endosc Clin N Am. 2008;18(1):11-23.
- Franciosi JP, Liacouras CA. Immunol Allergy Clin North Am. 2009;29(1):19-27.
- Müller S, Pühl S, Vieth M, et al. Endoscopy. 2007;39(4):339-344.
- Taft TH, Guadagnoli L, Edlynn E. J Asthma Allergy. 2019;12:389-399.
- Schoepfer AM, Safroneeva E, Bussmann C, et al. Gastroenterology. 2013;145(6):1230-1236.e1-2.
- Furuta GT, Katzka DA. N Engl J Med. 2015;373(17):1640-1648.
- Dellon ES, Kim HP, Sperry SL, et al. Gastrointest Endosc. 2014;79(4):577-585.e4.
- Reed CC, Corder SR, Kim E, et al. Am J Gastroenterol. 2020;115(6):853-858.
- Dellon ES. Gastroenterol Clin North Am. 2014;43(2):201-218.
- Rajan J, Newbury RO, Anilkumar A, et al. J Allergy Clin Immunol. 2016;137(1):147-156.e8.
- Clayton F, Peterson K. Gastrointest Endosc Clin N Am. 2018;28(1):1-14.
- O’Shea KM, Aceves SS, Dellon ES, et al. Gastroenterology. 2018;154(2):333-345.
- Hill DA, Spergel JM. Curr Allergy Asthma Rep. 2016;16(2):9.
- Simon D, Marti H, Heer P, et al. J Allergy Clin Immunol. 2005;115(5):1090-1092.
- Mohammad AA, Wu SZ, Ibrahim O, et al. J Am Acad Dermatol. 2017;76(3):559-560.
- Dellon ES, Hirano I. Gastroenterology. 2018;154(2):319-332.e3.
- Dellon ES, Jensen ET, Martin CF, et al. Clin Gastroenterol Hepatol. 2014;12(4):589-596.
- Dellon ES. Gastroenterol Clin North Am. 2013;42(1):133-153.
- Spergel JM, Book WM, Mays E, et al. J Pediatr Gastroenterol Nutr. 2011;52(3):300-306.
- Shaheen NJ, Mukkada V, Eichinger CS, et al. Dis Esophagus. 2018;31(8):1-14.
- Mansoor E. Dig Dis Sci. 2016;61(10):2928-2934.
- Harris JK, Fang R, Wagner BD, et al. PLoS One. 2015;10(5):e0128346.
- Carr S, Chan ES, Watson W. Allergy Asthma Clin Immunol. 2018;14(suppl 2):58.
- Alexander ES, Martin LJ, Collins MH, et al. Allergy Clin Immunol. 2014;134(5):1084-1092.
- Hirano I, Furuta GT. Gastroenterology. 2020;158(4):840-851.
- Menard-Katcher C, Henry M, Furuta G, et al. World J Gastroenterol. 2014;20(31):11019-11022.
- Gonsalves N. Dig Dis. 2014;32(1-2):89-92.
- Steinbach EC, Hernandez M, Dellon ES. J Allergy Clin Immunol Pract. 2018;6(5):1483-1495.
- Straumann A, Aceves SS, Blanchard C, et al. Allergy. 2012;67(4):477-490.
- Hirano I, Chan ES, Rank MA, et al. Gastroenterology. 2020;158:1776-1786.
- Bystrom J, O’Shea NR. Postgrad Med J. 2014;90(1063):282-289.
- Hirano I. Dig Dis. 2014;32(1-2):78-83.
- van Rhijn BD, Verheij J, Smout AJ, et al. Neurogastroenterol Motil. 2016;28(11):1714-1722.
- Ahmed M. World J Gastrointest Pharmacol Ther. 2016;7(2):207-213.
- Eluri S, Runge TM, Cotton CC, et al. Gastrointest Endosc. 2016;83(6):1142-1148.
- Hirano I. Gastroenterology. 2018;155:601-606.
- Collins MH, Martin LJ, Alexander ES, et al. Dis Esophagus. 2017;30(3):1-8.
- Grin A, Streutker CJ. Arch Pathol Lab Med. 2015;139(6):723-729.
- Saffari H, Peterson KA, Fang JC, et al. J Allergy Clin Immunol. 2012;130(3):798-800.
- Dellon ES, Jones PD, Martin NB, et al. Dis Esophagus. 2013;26(1):7-13.
- American Gastroenterological Association and the Joint Task Force on Allergy-Immunology Practice Parameters Clinical Guidelines for the Management of Eosinophilic Esophagitis. Management of eosinophilic esophagitis. GuidelineCentral.com. 2020.
- Aceves SS, Dellon ES, Greenhawt M, et al. Ann Allergy Asthma Immunol. 2023;130(3):371-378.
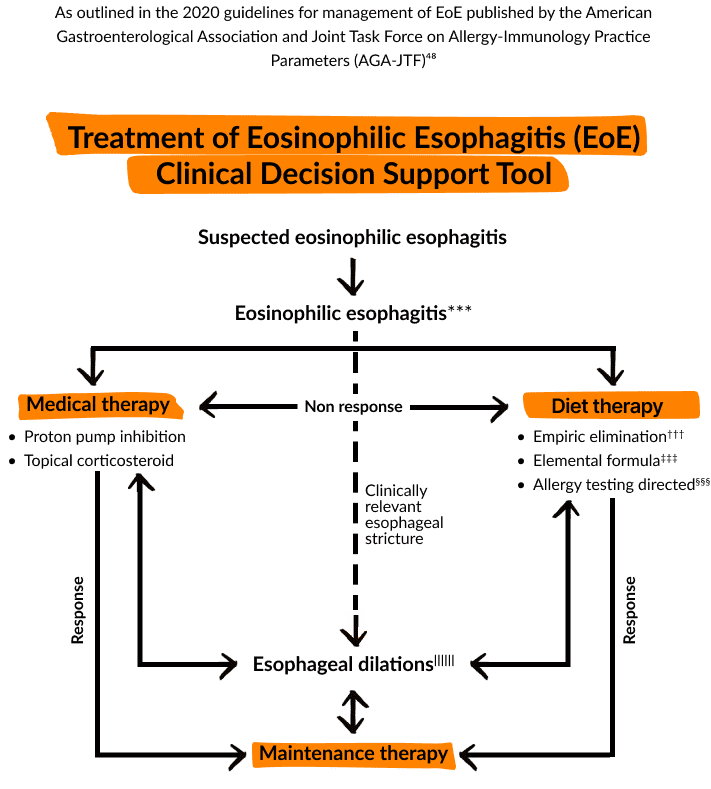
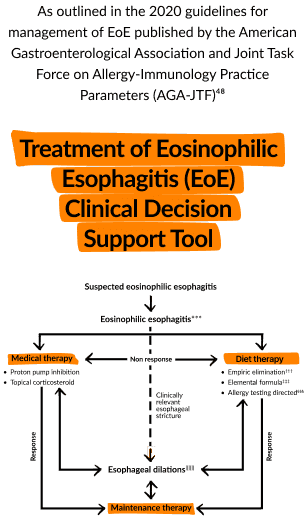
- Treatment of Eosinophilic Esophagitis (EoE): Clinical Decision Support Tool. Gastroenterology. 2020;158:1787.
- Eluri S, Iglesia EGA, Massaro M, et al. Dis Esophagus. 2020;33(7):doaa025.
- Drescher H, Lissoos T, Hajisafari E, et al. J Nurs Prac. 2019;15:676-681.
- Philpott H, Dellon ES. J Gastroenterol. 2018;53(2):165-171.
- Shah NA, Albert DM, Hall NM, et al. Clin Exp Gastroenterol. 2016;9:281-290.